Functional Architecture
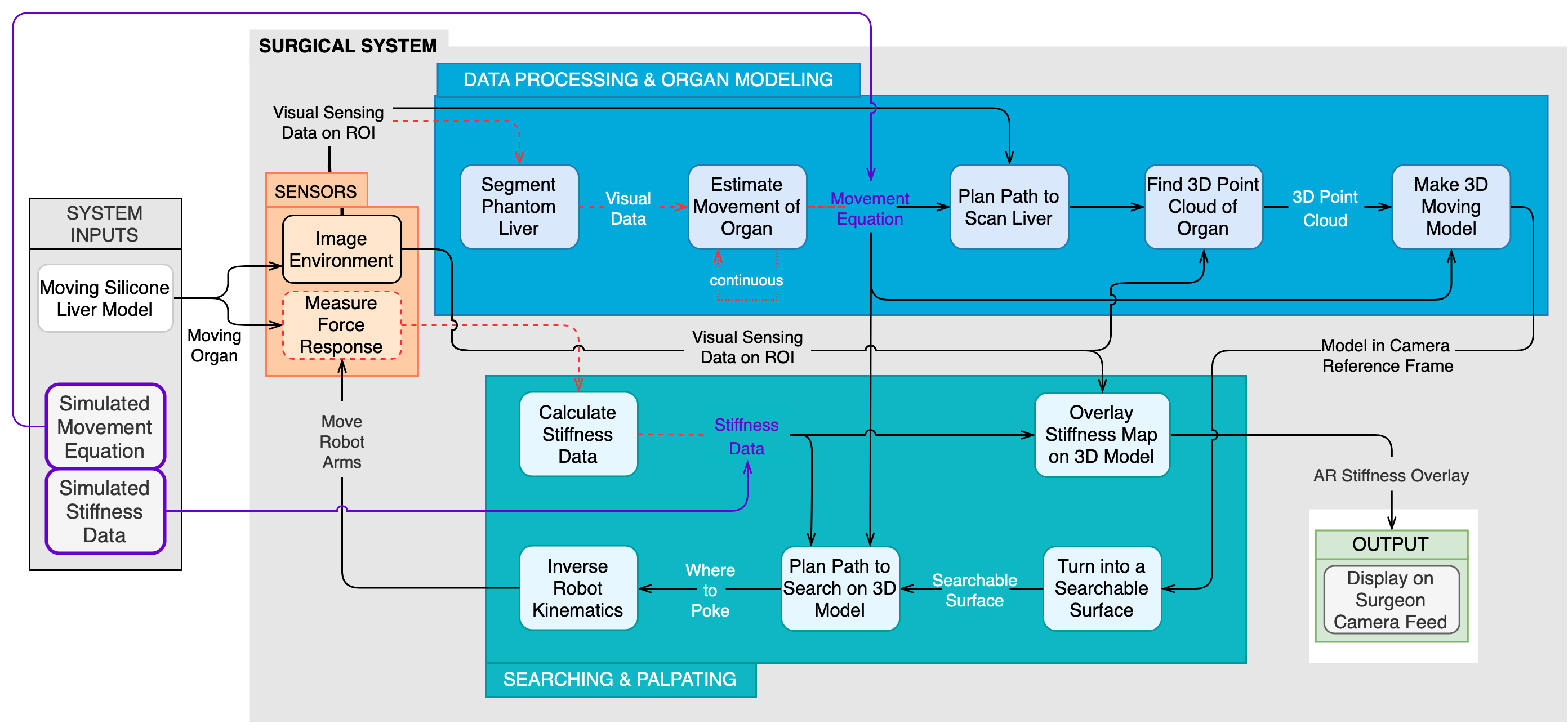
Cyberphysical Architecture
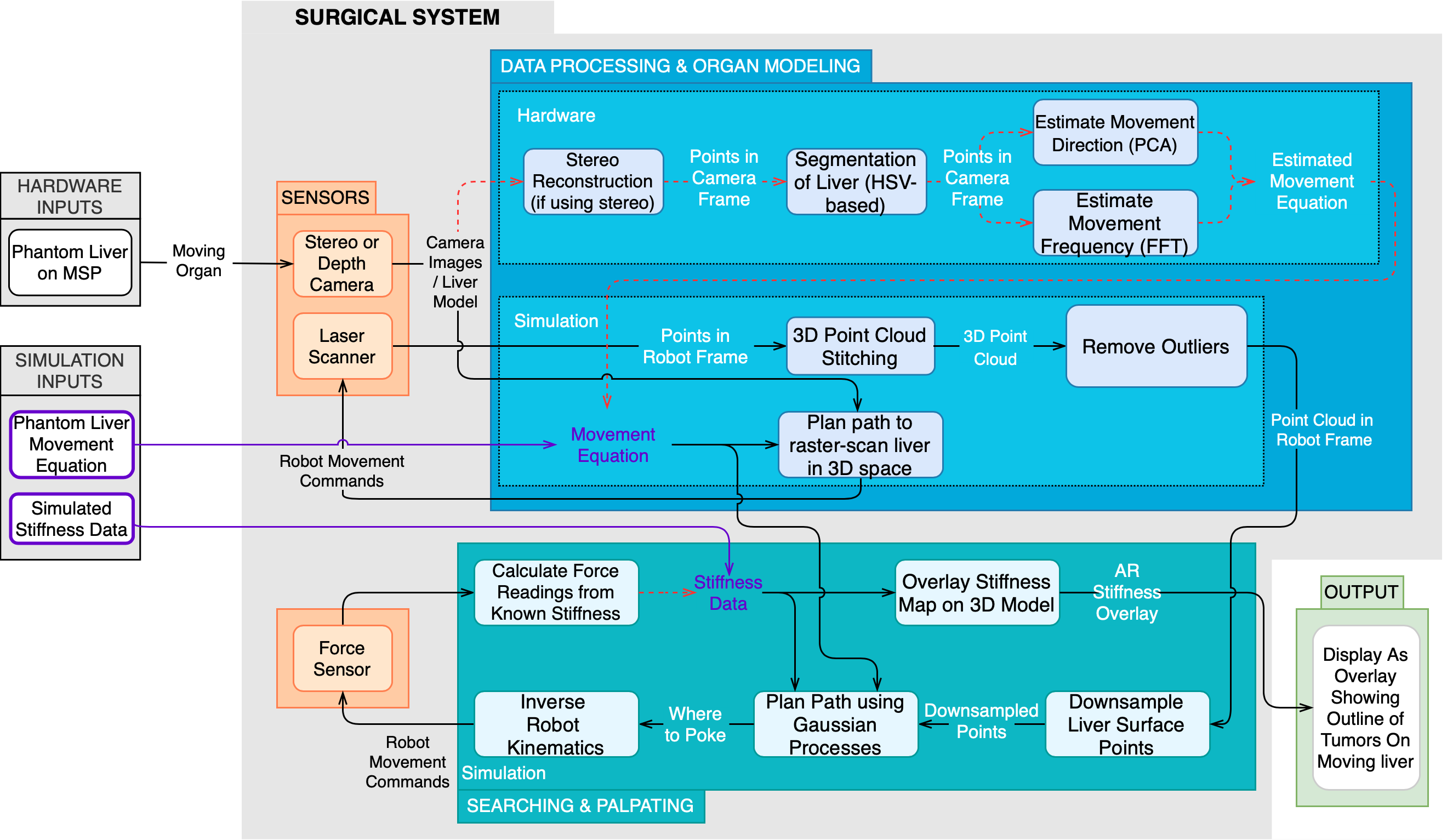
System Design Description
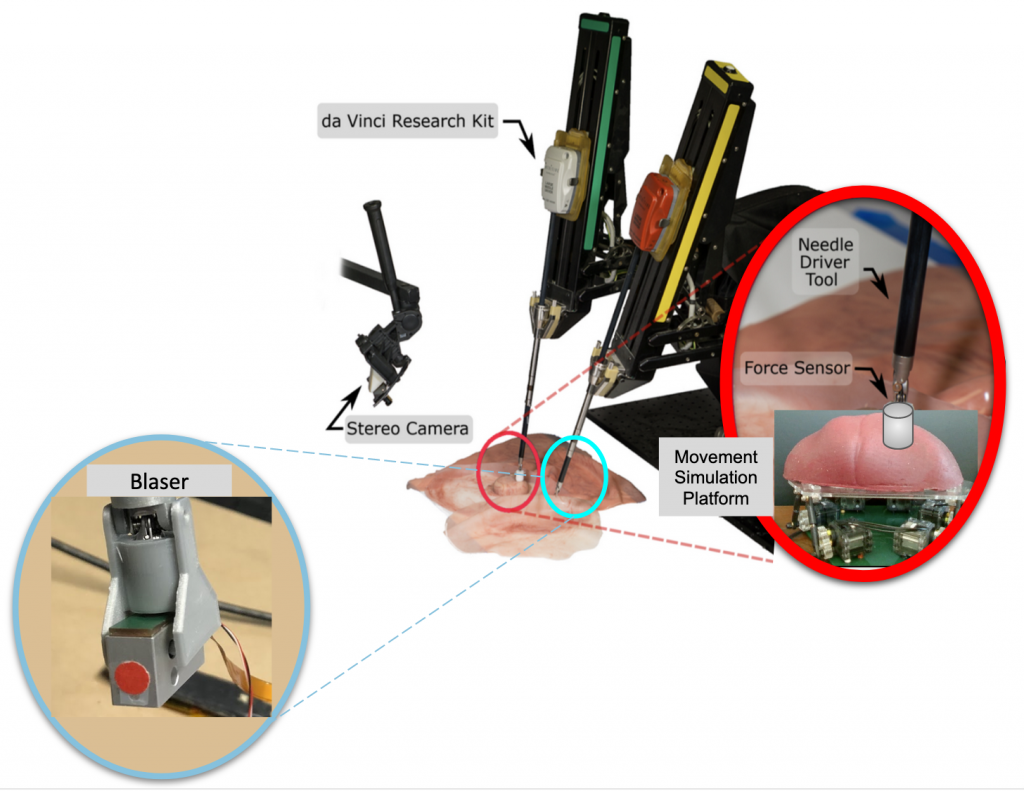
Figure 3: Depiction of the Chopsticks Surgical System
Sensors Subsystem
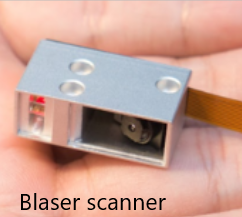


Figure 4: Main sensors of the Chopsticks Surgical System
Movement Simulation Platform
The purpose of the Movement Simulation Platform(MSP) is to simulate the motion pattern of the liver due to the patient’s respiration and heartbeat rhythm during surgery. It was built based on Professor Ken Goldberg’s Stewart Platform Research Kit for simulating organ motion for surgical robot prototypes. The MSP subsystem, which is a combination of software and hardware, has 6 degrees of freedom (DOF) to move and can rotate in 3D space. It can exhibit a translation of 1.27 cm along each of the x, y, and z axes, and a rotation of 15 degrees in roll, pitch, and yaw.
Hardware:
The main structure of the MSP was built in acrylic and actuated by 6 XL320 servo motors connected in series. The work surface was designed to be wide enough to contain the silicone models of the liver and other organs in its vicinity. The geometry of the hardware structure was developed such that it can support the weight of the silicon models above, and translate the rotational motion of the step motors into desired movements at the platform work surface.

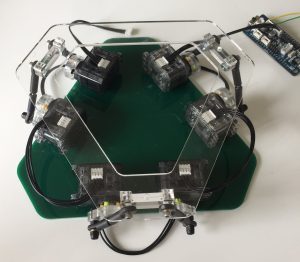
Figure 5: Movement Simulation Platform of the surgical system
Software:
The software interface provides an interface for the user to input different motion commands, and controls and estimates the movements of the step motors. The MSP is programmed in C via the onboard OpenCM 9.04-C microcontroller. In order to control the servo motors connected in series, commands are given in a form of [ServoID, Command Type, Command Goal].
Searching & Palpating Subsystem
This subsystem includes all the algorithms necessary to take a 3D model of an organ and output a stiffness map. This includes algorithms that transform the data to the correct form, search over the organ to detect tumors, control robot kinematics, and render the stiffness map.
Searchable Surface Transformation
There will be two main transformation algorithms. The first algorithm will take the 3D point cloud returned by the processing subsystem and convert it to a 3D searchable surface. This surface should be compatible with the current 3D Gaussian Process search algorithm developed by the lab.
Alternatives: We may instead convert the 3D point cloud into a 2D projection and do a 2D search on this surface. This simplifies the problem to a 2D search, which means it would not have to be compatible with the Biorobotics Lab’s original algorithm.
Force Reading Conversion
The second transformation algorithm will convert the force readings from the Blaser frame to the stereo camera frame. Since the 3D point cloud is in the stereo camera, this transformation is important to ensure the search algorithm correctly decides where to poke next in the stereo frame based on the force readings. The transformation was previously calculated in the data processing subsystem.
Force Reading to Stiffness Data
This algorithm will convert the readings from the force sensor into a Multivariate Gaussian Distribution that models the stiffness of regions of the organ based on the magnitude of the force readings. This means we will not have to poke the organ in as many locations because the readings can be generalized over the surface. This algorithm has been implemented by the lab so we do not anticipate needing an alternative. The force readings will be converted to stiffness data that indicate both the shape and location of tumors in the organ, and overlaid on the visual feed for the surgeon to see, as depicted in Fig. 3.
Search Over the Organ
The search algorithm will use active LSE to determine where the robot should poke the organ for maximum information gain. It will take the searchable surface and output coordinates in the robot frame of where to poke next.
Alternatives: Instead of intelligently determining where to poke the organ, the organ can be divided into a meshgrid and we can direct the robot to poke within each box of the grid in a brute-force manner.
Inverse Robot Kinematics
The dVRK already has PID control and robot kinematics implemented. The current robot kinematics allow the robot to move into “unreachable positions” from which the robot cannot recover. We will develop a helper algorithm on top of the robot kinematics to ensure that the robot does not move into these positions by checking if the desired position and orientation are within the operating range of the dVRK.
Display
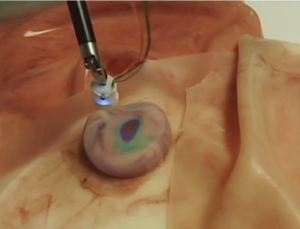
Figure 6: Stiffness map overlaid on phantom organ
Given a stiffness map, the Biorobotics Lab at CMU has implemented an algorithm to render it into stereo images. We will have to ensure that the stiffness map aligns with the moving organ. This will be done with rendering software with some preprocessing.
This subsystem works a little differently in simulation because we did not simulate a stereo camera. Once the robot completes the palpation procedure, a visualization of the results as shown in Figure 7 appears for the user/surgeon by switching on two ROS topics. The first topic publishes the shape and location of the ground truth tumor, shown in green, while the second topic publishes palpated points in white. During development, we overlay both visualizations on the liver to get an understanding of what percentage of the tumor(s) was classified correctly. The minimum bounding circle shown in yellow is sketched offline to show how we calculated our accuracy percentages.
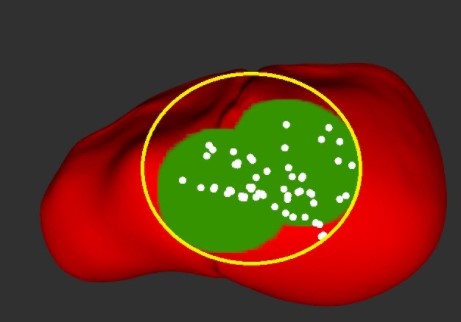
Figure 7: Stiffness map in simulation